
Medically Reviewed By
Dr. Kailash KothariMD Anesthesiology, Pain Medicine, FIAPM (Pain Medicine) · 30+ years experience
- No surgery required for many conditions
- Same-day procedures
- International training & advanced techniques
What is Epidural Steroid (cortisone) Injection ?
Epidural gluco-corticoid injections are commonly given to patients with leg and/or back pain to relieve such pain and improve mobility without surgery. These steroid injections buy time to allow healing to occur and/or as an attempt to avoid surgery after other conservative (non-surgical) treatment approaches have failed.
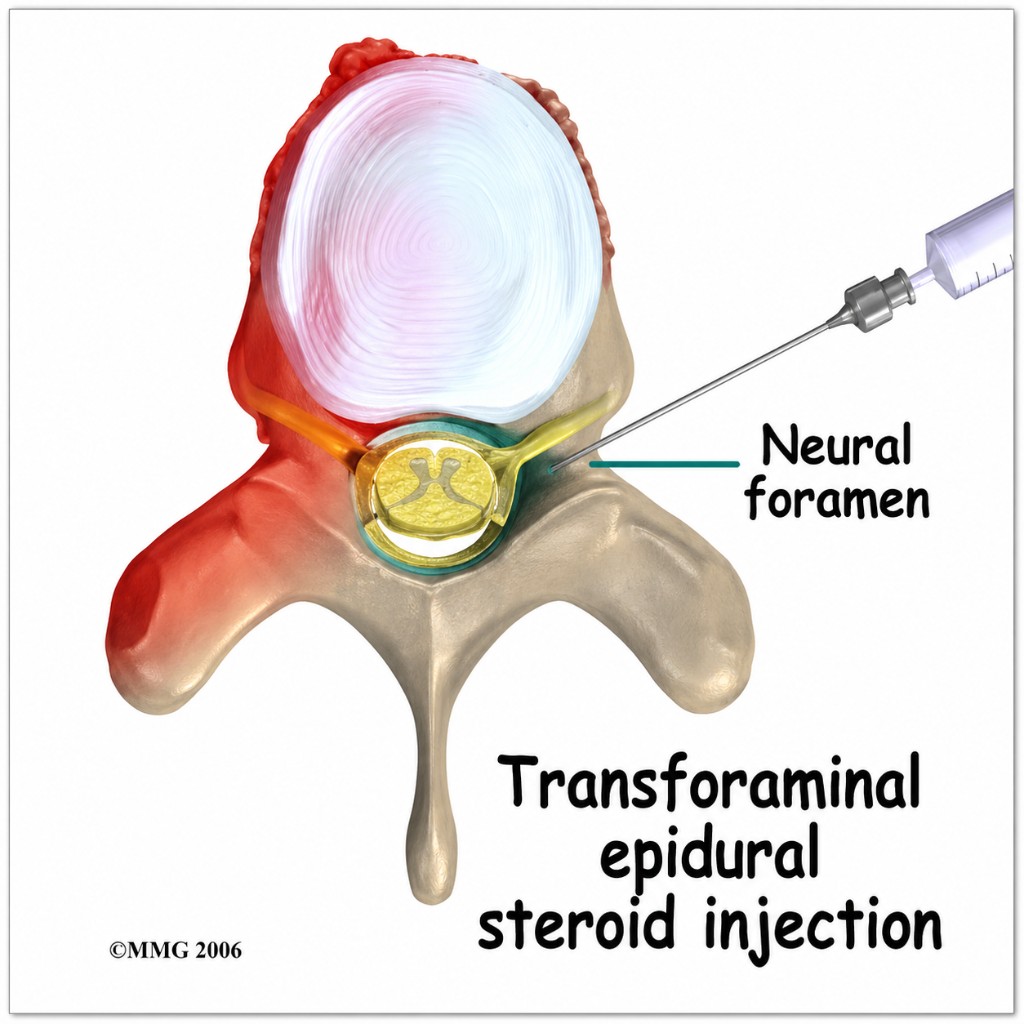
During a trans-foraminal injection, a thin needle is inserted into the epidural space through the bony opening of vertebral column from where a nerve root exits (neuroforamen). The drug is delivered exactly in the area where disc is compressing nerve and causing inflammation.
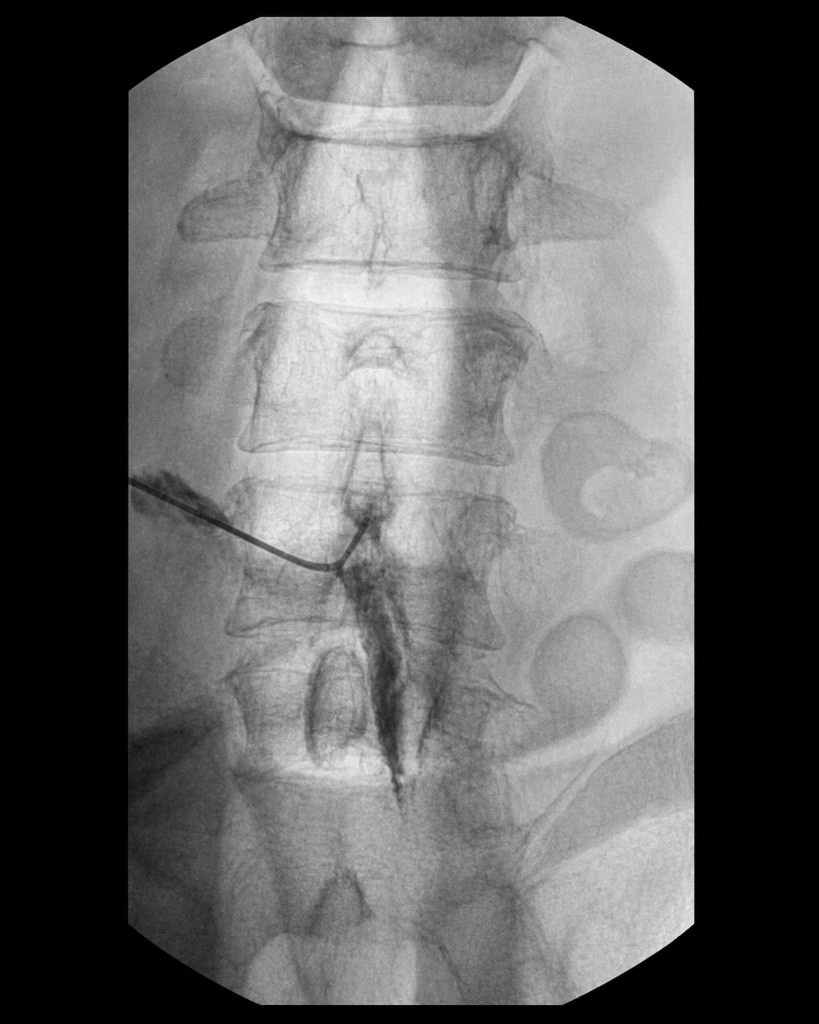
The procedure is performed with the patient lying on their belly using fluoroscopic (real-time x-ray) guidance, which helps to prevent damage to the nerve root. A radio-opaque dye is injected to enhance the fluoroscopic images and to confirm that the needle is properly placed (See Figure 2). This technique allows the cortisone medicine to be placed closer to the irritated nerve root. The exposure to radiation is minimal.
Indications include disc herniations, Lumbar canal stenosis, vertebral fractures, Cancer tumor compressing epidural space, Herpes zoster pain etc.
Patients with disc herniations and leg pain attains maximal improvement in 6 weeks. Interestingly, long-term success rates for trans-foraminal epidural glucocorticoid injections ranged from 71% to 84%.
Therapeutic Rationale – Why Steroids?
- Structures (pain generators) like nerves/discs are accessible to neural blockade.
- Surgery of these structure may fail to cure and may worsen painful spinal conditions.
- Degenerative processes of the spine and the origin of spinal pain is complex.
- The effectiveness of a large variety of therapeutic interventions used to manage chronic spinal pain has not been demonstrated conclusively.
- There is increasing evidence supporting the use of interventional techniques in managing spinal pain.
The Objective
- To deliver corticosteroid close to the site of pathology.
- Trans Foraminal Epidural Steroid Injection (TFESI) – more specific & targeted to site of pathology.
- Interlaminar injections are very effective in cervical (neck) area.
- Decrease size of disc means Decrease symptoms? It is not always the case, as compression may continue in spite of resolution of the symptom.
- In many cases MRI shows disc bulge but patients are pain free. It is also well described in many studies that asymptomatic individuals present with disc herniations that are evident on CT / MRI scans.
Multiple Mechanisms to Explain Radicular Pain
Nerve damage of various nature (Partial axonal damage, Neuroma formation, Focal demyelination, Intraneural edema), Impaired microcirculation, Chemical irritation, Inflammation. The Steroid acts to reverse all these.
Lumbar Epidural Steroid Injection

Cervical Epidural Injection
Epidural Injections Treatment Testimonial
“Complaint of Pain is cervical region since 6 Months MRI : Shows C6 – C7 disc prolapse.I have taken treatment at pain clinic of India Kalyan branch ---- I received epidural injection 1 Month back.Now pain has reduced above 70 %, now only exercises will settle pain completely. I am satisfied with epidural injection.”
— Dr. Vrushali R Khare
Who is Epidural steroid injections for disc prolapse for?
- Disc herniations with radicular pain
- Lumbar canal stenosis
- Vertebral fractures with epidural irritation
- Cancer tumour compressing epidural space
- Herpes zoster pain
- Patients with leg/back pain not improving on conservative treatment
How Epidural steroid injections for disc prolapse is performed
- Patient lies on the belly while fluoroscopic (real-time X-ray) guidance is used
- Thin needle is inserted into the epidural space through the neuroforamen
- Radio-opaque dye is injected to confirm proper placement
- Cortisone medicine is delivered close to the irritated nerve root
- This trans-foraminal approach targets the site where disc is compressing the nerve
Before, during & after the procedure
Before: Clinical evaluation and MRI review are completed first. If advised, blood thinners are adjusted and informed consent is taken.
During: The procedure is performed in prone position under fluoroscopic guidance. A contrast dye confirms exact position before medicine is injected. Radiation exposure is minimal.
After & recovery: Patients are observed briefly and usually discharged the same day. Maximal improvement in disc-herniation related leg pain is often seen in about 6 weeks.
Benefits of Epidural steroid injections for disc prolapse
- Relieves pain and improves mobility without surgery
- Targets medicine exactly near the compressed nerve root
- Long-term success rates reported from 71% to 84%
- Maximal improvement in many disc-herniation patients around 6 weeks
- Helps reverse inflammation, chemical irritation and intraneural edema
- Can avoid or delay surgery in selected patients
Risks & possible side effects
- Temporary soreness or mild flare-up at the injection site for 24–48 hours
- Transient numbness or weakness in the leg/arm from local anesthetic
- Post-dural-puncture headache (rare)
- Short-term blood sugar rise in diabetic patients
- Allergy to contrast dye or medication (very rare)
- Infection or bleeding (extremely rare with strict aseptic and image-guided technique)
Conditions treated with this procedure
Frequently asked questions about Epidural steroid injections for disc prolapse
Medical references
This page is informed by guidance from the following authoritative medical sources: